All may now find themselves suffering from phantom pains.
“My leg, it’s not there as anyone can plainly see.And yet, it pains me terrible sometimes.Even wakes me up at night.” – Ian Murray
Phantom Limb Pain: a phenomenon characterized by the experience of pain, discomfort, or other sensation in the area of a missing limb or other body part.
In fact, one does not have to lose a limb to suffer from Phantom Limb Pain. It also can occur with the loss of other body parts: eyes, tongue, nose, even breast.
The concept of phantom limb pain is not new. First described by the 16th Century French Military Surgeon Ambrose Pare, the term was first coined during the American Civil War by surgeon Silas Weir Mitchell. Up to 80% of patients who undergo amputation experience phantom limb pain with a range of symptoms including burning, shooting pain, “pins and needles,” twisting, crushing, electric shock feelings, itching, and vibration.
Why does Phantom Limb Pain occur?
In brief? The medical community don’t know exactly. There are a number of working theories.
One mechanism thought to be responsible for these symptoms is due to the direct trauma of the nerves themselves during amputation. The severed nerves grow and form groups of nerve cells called neuromas which then generate impulses that travel back to the central nervous system and are interpreted as pain.
Another theory suggests that the part of the brain cortex that normally receives input from that body area finds itself no longer receiving input. The cortex reorganizes and neighboring areas take over that part of the cortex. Because of this, pain impulses from areas of the body near the amputated limb are now interpreted as pain in the missing limb itself.
Or perhaps the symptoms are due to the lack of input. Deprivation of the normal perception of that limb causes abnormal signals to be transmitted which are interpreted as pain.
Whatever the exact mechanism (and there are likely more than one coming into play), unfortunately phantom limb pain remains a problem difficult to treat.
Treatment of Phantom Limb Pain
When possible, controlling pain prior to amputation can help. Phantom limb pain occurs more frequently in those who had significant pain in that area prior to amputation.
Medications including acetaminophen, NSAIDs, opioid medications (these are thought to diminish the cortical reorganization which is one of the potential mechanisms PLP develops), antidepressants, and anticonvulsants.
TENS (Transcutaneous Electrical Nerve Stimulation) has been found to be helpful for some.
Mirror Therapy is an interesting adjunct in treatment. Some theorize that the symptoms of Phantom Limb Pain are in part due to the absence of visual feedback about the limb to the brain. When a patient watches the reflection of their intact limb moving, the brain interprets it as the phantom limb moving, resolving the mismatch between the visual and sensory inputs about the limb.
Fortunately, the prevalence of phantom limb pain tends to decrease over time following the amputation.
What about broken hearts?
“Feeling a pain in a part of ye that’s lost. And thats just a hand. Claire was yer heart.” – Ian Murray
The pain of love lost. So similar. Jamie and Claire both feeling less than whole, the pain still raw, and a constant reminder of what they have lost.
If only there was an effective treatment for that…
The opening of The Garrison Commander finds Claire trying to assure the chivalrous Lieutenant Jeremy Foster that she is indeed a guest of the Clan MacKenzie and in no danger. Alas, he doesn’t seem fully convinced and informs Claire that she must accompany him to speak with his commander.
The Red Coats, Claire, and Dougal arrive in the village which Red Coats have occupied and Claire finds herself feeling some relief, sitting at a lovely meal of venison and charming her countrymen with lively conversation.
Her momentary relief is interrupted first by Captain Jack Randall (more to come) and then by a soldier who rushes in to inform the commander of an attack. Three enlisted men have been fired upon just outside of the camp. One man is dead, two are wounded, one severely, and no one can find the surgeon!
Claire, of course, is on her feet and ready to help.
Downstairs in the tavern, the wounded soldier is carried to a tavern table. His arm is significantly injured and Claire realizes it cannot be saved. The arm will need to be amputated. Claire takes charge, applying a tourniquet above the wound and instructing the men to bring boiling water and clean cloth.
The surgeon arrives and asks Claire whether she is going to faint when he begins to sew. He clearly doesn’t know our Claire. She assures him that she has seen worse and she directs the other soldiers to hold down the wounded man.
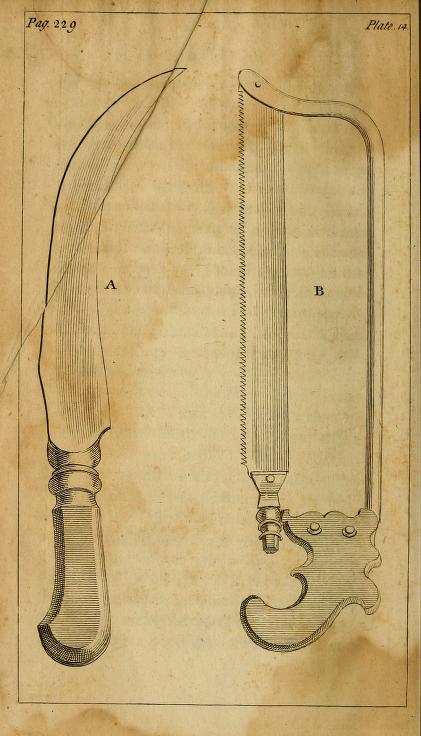
Having administered all available methods of anesthesia, the surgeon begins to saw.
The injured soldier is screaming, onlooking soldiers are sprayed with blood and in the corner, patrons of the tavern are still casually enjoying their ale.
The gruesome work begins / source: StarzSharp, Samuel. (1761). A treatise on the operations of surgery, with a description and representation of the instruments used in performing them: to which is prefix’d an introduction on the nature and treatment of wounds, abscesses, and ulcers. London: J and L Tonson. (source)
This tavern is far from the sterile operating rooms of today. Surgeries then took place often on kitchen tables with unwashed bare hands, dirty floors and tools that may have at most been wiped with a rag after their last use. It wouldn’t be until the second half of the 19th century that the work of Louis Pasteur, Joseph Lister, Robert Koch and others would revolutionize infection control.
In 1862, French chemist and microbiologist Louis Pasteur published his findings on the germ theory of infection, challenging the thinking of the time that infections were the result of “bad air” arising from rotting organic matter. In 1867, English physician Joseph Lister demonstrated a reduced mortality rate in his patients by using a carbolic acid on the tools and hands of the operating team as well as in the surgical wound.
Dr. William Stewart Halsted, surgeon at Johns Hopkins Hospital, adopted carbolic acid for antisepsis but it soon became clear that carbolic acid was quite rough on the hands of the surgical staff. In 1889 or 1890, Caroline Hampton, Halsted’s chief operating nurse, developed dermatitis on her hands from contact with the disinfectant. Halsted, who she would marry shortly thereafter, requested the Goodyear Rubber Company make her a pair of thin rubber gloves with gauntlets. They were such a success that within 10 years, surgeons and nurses alike were wearing them. Dr. Joseph Bloodgood, a protege of Halsted, published a report of a nearly 100% drop in infection rate from data on 450 hernia surgeries after he began routinely wearing surgical gloves.
In 1881, Robert Koch developed sterilization processes using steam and hot air and soon after, sterilization by boiling was introduced. Everything used during an operation from the tools to dressing and gowns were boiled.
These advances led to a marked decrease in post surgical infection and mortality. Prior to the introduction of aseptic techniques, most surgical wounds became infected and drainage of pus was actually expected. In fact, finding “laudable pus” – creamy yellow ooze – on a wound within the first 4 days was considered a sign of good healing. Mortality of surgical infections reached 70 percent. Today, with aseptic techniques in surgery and the use of antibiotics, the incidence of surgical site infection ranges from 2-7% with significantly lower rates of mortality.
It is unimaginable the pain these brave patients would have endured in these invasive surgeries with just a swig of opium and a bite block, if that.
Ancient methods of anesthesia for surgery included ingestion of opium or wine and herb mixtures, inhalation of opium and herbs from a sponge held near the nostrils and even application of cocaine by which Incan shamans chewed cocoa leaves and vegetable ash and let their cocaine-laden saliva drip into the wounds of their patients. It wasn’t until the 1800s that significant progress was made toward adequate anesthesia for surgery.
“Die Operation” by Gaspare Traversi, 1753. / source
Nitrous oxide was first discovered in 1772 by English Scientist Joseph Priestly when he tested it on himself, discovering that the gas made him laugh and would have possible anesthetic properties. In 1844, dentist Horace Wells volunteered to have one of his own teeth extracted under nitrous oxide. He then used it successfully over a dozen more times, and was invited by Dr. John Collins Warren at Massachusetts General Hospital to perform a public demonstration of its use for Warren’s students in 1845. Unfortunately, the gas was administered improperly and the patient cried out in pain and Wells was humiliated, ultimately committing suicide.
Dr. Warren, however, then invited Dr. William TG Morton to demonstrate the use of ether (diethyl ether gas, historically called “sweet vitriol”) to anesthetize a patient as he excised a small neck tumor. The patient remained unconscious throughout the procedure to the amazement of the audience. Thereafter, the use of inhaled anesthetics spread and evolved so that now, the 18 gauge needle used to start an IV in the pre-op holding area might be the most painful part of a surgery!
Later in the episode, Claire is alone with Black Jack Randall. A long discussion could be had about his psychiatric condition, but for today, we’ll discuss the brutal punch he gave Claire and the kicks that he ordered Corproral Hawkins to administer to Claire. Hit directly in the abdomen, Claire has suffered diaphragm spasm, or more commonly, she had the wind knocked out of her.
When we inhale, the diaphragm contracts, drawing the lungs down and expanding the rib cage. A temporary vacuum is created and air is pulled through the nose and mouth into the lungs. In exhalation, the diaphragm relaxes, the lungs deflate, and air is expelled out of the mouth and nose. A strong kick to the abdomen causes the diaphragm muscles to spasm, unable to contract and relax normally and thus leaving the victim unable to draw a breath. While it is terrifying and panic inducing, having the wind knocked out of you is not life threatening, and resolves on its own in a few moments.
Dougal rushes in and saves Claire, leaving Randall under the impression that Claire will be delivered to Fort William before sundown tomorrow.
After proving she is not a spy when her gizzards are not burned out at St. Ninian’s spring, Dougal presents to Claire his plan for keeping her out of the hands of the English. The episode ends with Claire downing a bottle of whisky as she considers the prospect of marrying a strapping young Scot.